The cranial nerves associated with the orbit are CN II (vision), CN III (eye movement), CN IV (eye movement), CN V-1 (general sensory to eye and scalp), CN VI (eye movement), and CN VII (crying and closing the eyes).
CN II: Optic Nerve
The optic nerve enters the orbit through the optic canal along with the ophthalmic artery and provides special sensory innervation (vision) from the retina to the brain. CN II from one eye joins CN II from the corresponding eye to form the optic chiasma.
CN III: Oculomotor Nerve
The oculomotor nerve emerges from the midbrain and courses anteriorly between the posterior cerebral and the superior cerebellar arteries, through the lateral wall of the cavernous sinus and superior orbital fissure into the orbit, where the nerve bifurcates into superior and inferior divisions (Figure B and C). The oculomotor nerve (III) innervates the medial, inferior, and superior rectus muscles and the inferior oblique muscle.
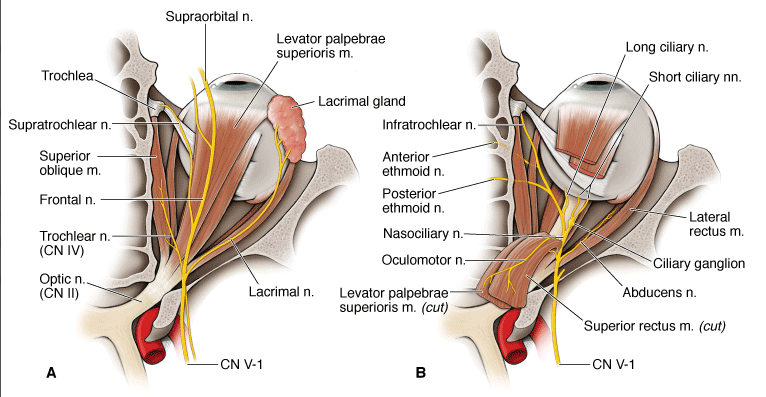
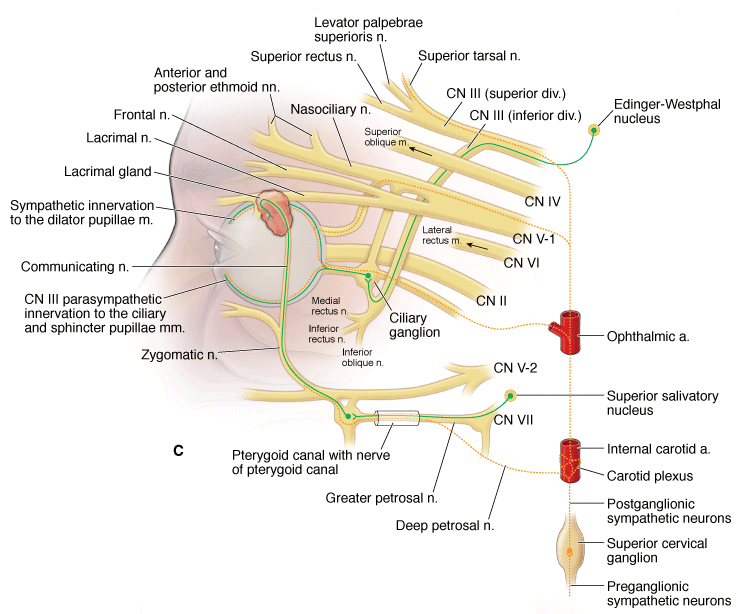
Superior view of the nerves of the orbit (A. superficial). (B. deep). C. Comprehensive innervation of the orbit highlighting autonomics.
- Superior division. Provides somatic motor innervation to the levator palpebrae superioris and superior rectus muscles.
- Inferior division. Provides somatic motor innervation to the medial rectus, inferior rectus, and inferior oblique muscles. CN III also provides visceral motor innervation. Preganglionic parasympathetic neurons originate in the Edinger–Westphal nucleus and course in the inferior division of CN III and synapse in the ciliary ganglion (between CN II and the lateral rectus muscle). Postganglionic parasympathetic neurons course in the short ciliary nerves to enter the eyeball and innervate the ciliary muscles (lens accommodation) and pupillary sphincter muscles (pupil constriction).
 Injury to CN III results in a fixed, dilated pupil because the dilator pupillae muscle no longer has an antagonistic muscle counteracting its force. The lens does not accommodate (due to loss of innervation to the ciliary muscles) and ptosis develops (due to loss of innervation to the levator palpebrae superioris muscle). Because of the unopposed action of the lateral rectus and superior oblique muscles, the eye deviates to the abducted and down and out position.
Injury to CN III results in a fixed, dilated pupil because the dilator pupillae muscle no longer has an antagonistic muscle counteracting its force. The lens does not accommodate (due to loss of innervation to the ciliary muscles) and ptosis develops (due to loss of innervation to the levator palpebrae superioris muscle). Because of the unopposed action of the lateral rectus and superior oblique muscles, the eye deviates to the abducted and down and out position.
CN IV: Trochlear Nerve
The trochlear nerve arises in the midbrain and is the only cranial nerve to exit from the posterior surface of the brainstem. After curving around the midbrain, CN IV courses through the lateral wall of the cavernous sinus to enter the orbit via the superior orbital fissure (Figure A). CN IV provides somatic motor innervation to the superior oblique muscle.
Injury to CN IV results in the inability to view an object inferiorly when the eye is adducted.
CN V-1: Ophthalmic Branch of the Trigeminal Nerve
The ophthalmic nerve courses through the superior orbital fissure and provides general sensory innervation to the orbit via the following three branches (Figure 18-4A–C):
- Lacrimal nerve. Innervates the lacrimal gland, conjunctiva, and skin of the upper eyelid.
- Frontal nerve. Courses superior to the levator palpebrae superioris muscle and bifurcates into the supraorbital and supratrochlear nerves to innervate the skin of the forehead and scalp.
- Nasociliary nerve. Provides general sensory innervation via the following branches:
- Long ciliary nerves. Supplies the cornea (sensory limb of the pupillary reflex).
- Posterior ethmoidal nerve. Supplies the sphenoid and ethmoidal sinuses.
- Anterior ethmoidal nerve. Supplies the ethmoid sinus, nasal cavity, and skin on the tip of the nose.
- Infratrochlear nerve. Supplies the lower eyelid, conjunctiva, and skin of the nose.
CN VI: Abducens Nerve
The abducens nerve enters the orbit via the superior orbital fissure and provides somatic motor innervation to the lateral rectus muscle (Figure B). The abducens nerve (VI) innervates the lateral rectus muscle.
Injury to CN VI results in the inability to abduct the eye, resulting in diplopia and loss of parallel gaze.
In the orbit, the facial nerve “makes you cry” (visceral motor) and “close your eyes” (branchial motor) (Figure 18-4C).
- Preganglionic parasympathetic neurons from CN VII originate in the superior salivatory nucleus (pons) and exit the cranial cavity through the internal acoustic meatus. At the geniculate ganglion, CN VII gives off the greater petrosal nerve, which joins with the deep petrosal nerve (sympathetics from the carotid plexus), becoming the nerve of the pterygoid canal (Vidian nerve). The nerve of the pterygoid canal enters the pterygopalatine fossa, where preganglionic parasympathetic neurons synapse in the pterygopalatine ganglion. Postganglionic parasympathetic neurons join with the zygomatic nerve (CN V-2) and then with the lacrimal nerve (CN V-1) to innervate the lacrimal gland.
- CN VII provides branchial motor innervation to the orbicularis oculi muscle.
Sympathetics to the orbit course in the following pathways (Figure 18-4C):
- Postganglionic sympathetic neurons originating in the superior cervical ganglion ascend along the internal carotid artery up to the ophthalmic artery.
- Sympathetic nerves innervate the superior tarsal muscle (keeping the eyelid open) and the dilator pupillae muscles.
- Sympathetic nerves innervate the superior tarsal muscle (keeping the eyelid elevated) and the dilator pupillae muscles.